In NEJM Knowledge+ Internal Medicine Board Review, we have a number of questions about managing patients with suspected bacterial meningitis, and these tend to generate comments from our learners. How do you balance the need to give antibiotics rapidly with the time needed to obtain required diagnostic studies?
Evaluation and Treatment for Most Patients with Suspected Bacterial Meningitis
In general, most patients who present with features of bacterial meningitis, such as fever, headache, and nuchal rigidity, should have blood tests obtained immediately, including blood cultures. These tests should be followed by a lumbar puncture for cerebrospinal fluid (CSF) analysis. Typically, these studies can be obtained rapidly, and the results will be immensely helpful in tailoring therapy.
Once the samples have been obtained, empiric antibiotic therapy is started. The Infectious Diseases Society of America (IDSA) recommends that empiric treatment be tailored to the patient’s age and comorbidities (especially the presence of immunosuppression). Empiric therapy in otherwise healthy adults should cover Streptococcus pneumoniae, Neisseria meningitidis, group B Streptococcus, and Haemophilus influenzae. Such coverage can be achieved with vancomycin plus a third-generation cephalosporin such as ceftriaxone or cefotaxime, with the addition of ampicillin in adults older than 50 years of age in whom Listeria monocytogenes is an additional pathogen to consider. Once the microscopic examination of the CSF (including a Gram stain) and the culture results from the blood cultures and CSF return, the antibiotic therapy can often be matched to a specific pathogen.
In addition, dexamethasone is recommended in patients in whom S. pneumoniae is suspected as it has been shown to reduce the risk of neurologic sequelae. Dexamethasone should be administered at the same time as the antibiotics, but the causative organism is often not known at that time. However, because S. pneumoniae is the most common cause of meningitis in the United States, dexamethasone is typically given to all patients with suspected meningitis — and then discontinued if S. pneumoniae is not isolated from the blood or CSF.
In short, the typical order is: Blood cultures ➔ lumbar puncture ➔ antibiotics/steroids.
When to First Perform a CT of the Head
Not all patients can proceed directly to a lumbar puncture. This procedure carries a risk of brain stem herniation and death in patients with elevated intracranial pressure; therefore, patients at risk of elevated intracranial pressure require a CT of the head before proceeding.
The IDSA recommends that a CT be obtained before lumbar puncture in the following groups of patients:
- Patients who are immunocompromised (HIV infection, taking immunosuppressants, or after transplantation)
- Patients with a history of central nervous system disease (mass lesion, stroke, or focal infection)
- Patients with new onset of seizure within one week of presentation
- Patients with papilledema on fundoscopy
- Patients with an abnormal level of consciousness
- Patients with a focal neurologic deficit
The following decision tree from the IDSA guideline may be helpful:
Management Algorithm for Adults with Suspected Bacterial Meningitis
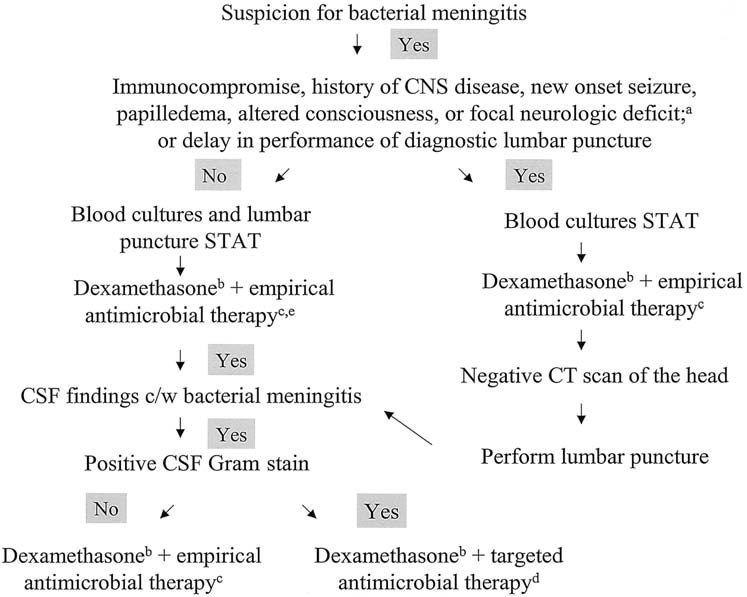
“STAT” indicates that the intervention should be done emergently.
- See table 2 of IDSA Guidelines.
- See text of IDSA Guidelines for specific recommendations for use of adjunctive dexamethasone in adults with bacterial meningitis.
- See table 4 of IDSA Guidelines.
- See table 3 of IDSA Guidelines.
- Dexamethasone and antimicrobial therapy should be administered immediately after CSF is obtained.
What if Obtaining a CT Scan Would Take Too Long?
In most care settings, obtaining a CT scan is a time-consuming task. If antibiotic therapy is delayed until after a CT scan and the subsequent lumbar puncture has been obtained, there is a greater likelihood of delays of up to 6 hours before antibiotics are administered, with resulting worsened patient outcomes. Therefore, in patients who require a CT before a lumbar puncture can be performed safely, it is better to give antibiotics before obtaining the CT.
In other words, whereas the typical order is: blood cultures ➔ lumbar puncture ➔ antibiotics/steroids, the order should be altered in patients who need a CT to be: blood cultures ➔ antibiotics/steroids ➔ CT ➔ lumbar puncture.
There are some drawbacks to providing antibiotics before obtaining the lumbar puncture. The primary concern is that the yield of the CSF Gram stain and culture may be reduced — results of CSF white blood cell count, glucose, and protein do not change rapidly. Studies have shown that, even though the yield of CSF Gram stain and culture is reduced in patients who receive antibiotics before lumbar puncture is performed, the Gram stain and culture can remain positive and allow identification of the pathogen for several hours after the administration of antibiotics. The slightly reduced yield is a small price to pay if lives can be saved and disability prevented thanks to earlier antibiotic therapy.
When to Give Antibiotics Early
There are times where antibiotics may be administered early even if a CT is not needed. If there are delays in obtaining blood cultures or lumbar puncture — typically, a delay of more than one hour — then antibiotics should be administered even though the diagnostic evaluation is not yet completed.
Putting Knowledge into Practice
Evaluating patients with suspected bacterial meningitis can be challenging, particularly determining the appropriate sequence of events. We hope that the guideline-based information we have provided is helpful.
What types of challenges have you encountered with suspected bacterial meningitis in your own practice?
 Ole-Petter Riksfjord Hamnvik, MB BCh BAO, MMSc is an endocrinologist at Brigham and Women’s Hospital; Program Director, Endocrinology Fellowship at BWH; and Education Editor, NEJM Group.
Ole-Petter Riksfjord Hamnvik, MB BCh BAO, MMSc is an endocrinologist at Brigham and Women’s Hospital; Program Director, Endocrinology Fellowship at BWH; and Education Editor, NEJM Group.
I am a general pediatrician and did my residency from 1979 – 1982. Bacterial meningitis in children – I know this discussion deals more with adults but there are parallels – was far more common then than now. Our Chair would buy us a 6-pack of our favorite beverage if we could complete the ER work-up and therapy in less than 30 minutes from the time you opened the door to the patient’s room. Everything had to go beautifully well. Blood had to be drawn with the first stick, LP had to be successful with the first stick, and the IV had to be obtained on the first stick. Antibiotics were kept in the ER and we had to have all this done and the antibiotics infusing in less than 30 minutes. Didn’t happen open but it certainly taught us that therapy should not be delayed.
Microbiology services are not optimum, and , sometimes lacking in several parts of the world: therefore antibiotic therapy should not be delayed if microbiology services are not readily available.
as lab survice is not round the clock to start antibiotic early is m choice.
The CT before LP to “prevent” brainstem herniation is a myth and must be slain!!!!
Never ever been shown.
We can disprove this axiom by knowing a little anatomy (first year medical student) and physics as known to high school students. No special, secret knowledge needed.
Then we will prove it by reverse engineering.
If a patient does not have signs of elevated ICP, they do not have elevated ICP. Nice literature review: https://www.mdedge.com/internalmedicinenews/article/128706/infectious-diseases/myth-month-ct-scan-lumbar-puncture-suspected.
If a patient has communicating hydrocephalus with elevated ICP, then the fluid pressure will transmit through Aqueduct of Sylvius and through Foramina of Luskka into the spinal colmunmn’s subarachnoid space. There can be no herniation without occlusion of one of these foramina and performance of the LP cannot physically cause such a shift.
Reverse engineering: What is an accepted treatment modality for known elevated ICP? Spinal tap. No CT required.
So let’s get our learning evidence and logic based and start slaying myths. Or at least stop teaching them.
Your comment was almost perfect. You should have ended it with “Can I get an amen from the congregation?” I would gladly have given it!
Bacterial meningitis can be extremely dangerous. I recall we lost one adult patient 20 minutes after she entered the ER. Another patient, school age boy, came to my office and had petechiae and meningeal signs. I went to the ER did a surgical cutdown to have a secure IV, got blood culture and started antibiotics. I was criticized by an internist because I didn’t call a surgeon to do the cutdown (there were a lot of “privileges” issues at this hospital). He did well. During residency a young woman with near term pregnancy entered the hospital with headache. The intern suspected CNS problem and funduscopic showed signs of increased CNS pressure. Because of the risk of doing LP a neurosurgeon was called. The spinal fluid revealed evidence of Cryptococcus on india ink prep. She was sent immediately to a university hospital for treatment. A few days later we read her obituary in the local paper that stated she was survived by her baby daughter.
These cases illustrate that there can be no delay in establishing treatment because of the possibility of a rapidly fatal outcome. The case of cryptococcal disease happened before the era of AIDS but all cases of suspected meningitis should have the india ink prep. Also if WBC’s are found in CFS but gram stain and culture are not positive the patient should be evaluated for tuberculous meningitis. Choice of initial empirical antibiotic therapy is based on age and immune status: neonate, infant: child, adult, immunity impaired.
Thanks to everyone for your comments!
The post deals specifically with management in a typical US hospital, where microbiology services are available. In many cases, management in more underserved settings needs to be adapted. However, even if the lab is not available around-the-clock, a sample can be processed the next day so it would still be beneficial to obtain the sample.
As far as the need for a CT scan – it would be difficult to defend an adverse outcome from an LP if a CT scan was not obtained, as it is still considered the standard of care in patients with evidence of elevated ICP. The IDSA guidelines nicely discusses the evidence base for their recommendation (https://academic.oup.com/cid/article/39/9/1267/402080).