
Every week for the past 7 months, we’ve emailed NEJM Knowledge+ IM board review questions to thousands of physicians and residents as part of our NEJM Knowledge+ Question of the Week initiative. Some of the recipients are preparing for their board exams, and some are looking to maintain their knowledge base, but one thing is certain: they’re all looking for a challenge, and so far, NEJM Knowledge+ seems to be delivering.
Of the 29 questions we’ve emailed out so far, just over half were answered correctly by the majority of respondents.
When one of our questions is answered incorrectly by a large number of individuals, we take a close look to make sure the question is indeed consistent with the current standard of medical care and that we have not inadvertently created a trick question with our wording choices. We also read each and every comment we receive about our questions, as those comments often provide clues about which elements of a question might have been problematic. If revisions to a question are necessary, we make them immediately and incorporate them into NEJM Knowledge+, so that users are always seeing the latest version of our content.
Let’s take a look at some of our most challenging questions to date.
Interpreting Blood Pressure
On August 12, we asked participants to interpret the 24-hour ambulatory blood pressure readings of a 49-year-old man and determine the most appropriate next step in his care. As shown below, only 23% correctly diagnosed the patient as hypertensive and chose to initiate medical therapy; most respondents opted for lifestyle modification instead.
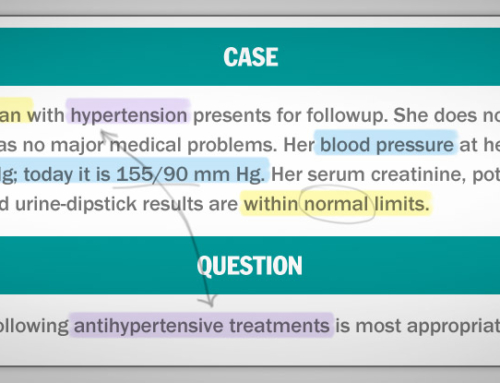
What is the most appropriate management approach for an asymptomatic 49-year-old man with a BMI of 32, in-clinic blood pressure readings of 148/90 mm Hg and 150/94 mm Hg, and a 24-hour average ambulatory blood pressure recording of 142/88 mm Hg?
a) Diagnose hypertension and initiate medical therapy (23%)
b) Diagnose hypertension and initiate lifestyle modification (24%)
c) Diagnose prehypertension and initiate lifestyle modification (47%)
d) Reassure the patient that the findings are normal (3%)
e) Repeat the ambulatory blood pressure monitoring (3%)
This pattern of responses likely reflects the controversy that has surrounded the JNC 8 directives since they were released in late 2013. The directives recommend initiating antihypertensive therapy in patients younger than age 60 who have an ambulatory blood pressure of ≥140/90 mm Hg. However, some experts have argued that this recommendation is not evidence-based and will result in overtreatment. The hypertension debate continues, but in the meantime, our hypertension questions will continue to be based largely on the JNC 8 guidelines that establish the standard of care.
Recognizing Brain Abscess
On September 9, we asked readers to identify the most likely diagnosis in an afebrile man who had a headache and focal neurologic signs that had been gradually progressing for the past 2 days. Only a quarter of respondents correctly concluded that these signs and symptoms were suggestive of a brain abscess; most people thought the patient was having a stroke.
Which one of the following diagnoses is most likely for an afebrile 40-year-old patient with headache and gradually progressive focal neurologic signs that evolve over 2 days?
a) Brain abscess (26%)
b) Bacterial meningitis (2%)
c) Acute stroke (47%)
d) Viral encephalitis (15%)
e) Toxic metabolic encephalopathy (10%)
Although focal neurologic signs can progress in both an abscess and a stroke, the speed of the progression is what helps to differentiate between the two. Symptom onset over seconds or minutes suggests a vascular event, whereas onset over several hours or days suggests an abscess; progression over an even longer period (weeks to months) would suggest a neoplasm.
Recognizing Gonococcal Arthritis
On September 16, we challenged readers to recognize that disseminated gonococcal infection can manifest as arthritis. About a third of respondents correctly considered gonoccocal arthritis the leading diagnosis and chose cervical nucleic acid amplification testing as the most appropriate next step in evaluation. The more common response, though, was to test for arthritis related to connective-tissue disorders. However, these disorders typically manifest as polyarticular arthritis rather than the monoarticular arthritis seen in this case patient.
Which one of the following diagnostic approaches is most appropriate for a woman with migratory arthralgias and a neutrophilic knee effusion whose synovial fluid is clear and tests negative on Gram’s stain and culture?
a) Cervical nucleic acid amplification assay (31%)
b) Antinuclear antibody testing and rheumatoid-factor testing (43%)
c) Complement CH50 blood testing (7%)
d) Parvovirus serology testing (17%)
e) Factor VIII testing (2%)
“Distractors” Do Their Job
As you’ve seen by now, all the questions in NEJM Knowledge+ offer five answer options – the correct choice plus four “distractors,” options that are plausible but incorrect because of an important and often subtle nuance. In NEJM Knowledge+, we pride ourselves on creating solid distractors, the kind that really test your knowledge of the details and the sort that you’re likely to find on the ABIM board exam. The best way to improve your performance on IM board review questions is to use specific board exam test strategies and to take lots of practice questions.
In the examples below, the correct answer always won out, but other answer choices made a respectable showing, indicating that our distractors did their job well for Question of the Week respondents.
Managing a Staphylococcus aureus Skin Abscess
On June 3, we asked readers to choose the most appropriate management for a skin abscess that was caused by community-acquired methicillin-resistant Staphylococcus aureus (MRSA) and not accompanied by any systemic symptoms or cellulitis. Exactly half of respondents correctly identified incision and drainage alone as the most appropriate management in this case, but a full 30% chose cephalexin plus incision and drainage.
Which one of the following management approaches is most appropriate for a skin abscess caused by community-acquired methicillin-resistant Staphylococcus aureus without associated systemic symptoms or cellulitis?
a) Incision and drainage of the abscess (50%)
b) Dicloxacillin (7%)
c) Cephalexin (3%)
d) Trimethoprim–sulfamethoxazole (10%)
e) Cephalexin plus incision and drainage of the abscess (30%)
Antibiotic therapy is an appropriate part of abscess management if the patient has systemic symptoms or signs, extensive involvement (such as multiple abscesses), or significant or rapidly progressing cellulitis. However, this case had none of those features; even if it did, cephalexin would not be an appropriate option because it does not have activity against MRSA.
Predicting Electrolyte Changes in a Hyperglycemic Emergency
On July 8, we described a patient in a hyperosmolar hyperglycemic state and asked which electrolyte changes would be expected to occur once a continuous intravenous insulin infusion was initiated. More than 80% of respondents correctly noted that the serum potassium level would fall, but a substantial proportion missed that, at the same time, the serum sodium level would rise.
Which one of the following sets of electrolyte changes would be most likely to occur after initiation of a continuous intravenous insulin infusion in a patient who is in a hyperosmolar hyperglycemic state?
a) An increase in the serum sodium level and a decrease in the serum potassium level (48%)
b) A decrease in the serum sodium and potassium levels (37%)
c) An increase in the serum sodium and potassium levels (3%)
d) A decrease in the serum sodium level and an increase in the serum potassium level (6%)
e) No change in the serum sodium level and an increase in the serum potassium level (6%)
The explanation for those rising sodium levels? As blood glucose corrects with the administration of a continuous intravenous insulin infusion, the serum osmolality rapidly drops, and the water that moved out of the cells in response to hyperosmolality now reenters the cells, thereby increasing the serum sodium level. Thus, the serum sodium level is expected to rise with the correction of the serum glucose.
Some IM Board Review Questions Prove to Be Less Difficult
Of course, not all of the NEJM Knowledge+ Questions of the Week are difficult. Here are some of the topic areas where respondents excelled:
- Nearly 80% of readers correctly recognized that the arm weakness and Horner’s syndrome seen in a 65-year-old former smoker were consistent with a diagnosis of an apical bronchogenic cancer known as a Pancoast’s tumor.
- Nearly 80% of readers correctly recognized inflammatory bowel disease–associated arthritis in a young woman with pain, stiffness, swelling, and a recent diagnosis of Crohn’s disease.
- More than 70% of readers correctly opted to evaluate for allergic bronchopulmonary aspergillosis in an elderly man who had recurrent asthma exacerbations, patchy opacities with central bronchiectasis on chest radiography, an elevated immunoglobulin E level, and eosinophilia.
Weekly IM Board Review Questions Help You Learn
NEJM Knowledge+ Question of the Week provides a worthy challenge to test your core knowledge of internal medicine topics, drawing from our question bank of thousands of case-based questions across a range of subspecialties, settings, and patient demographics. If you haven’t seen a question yet in your subspecialty, you will. We aim to ensure that our questions are not only accurate and clear but also relevant to your clinical practice.
Challenge yourself by signing up for NEJM Knowledge+ Question of the Week — it’s free and it’s fun! And if you’ve already signed up, let us know what you think of our questions and what we can do better. We’re certainly up for the challenge.
Want more? NEJM Knowledge+ Internal Medicine Board Review includes more than 1,500 case-based questions just like these! And it serves them up in multiple alternate formats on an adaptive platform that responds to your strengths and weaknesses and your reported confidence in each answer to help you consistently improve and retain your knowledge. See a demo here.
More from the Learning+ Blog:
How to Keep Up with Guidelines for ABIM Boards
Screening for HBV Infection: A Follow-Up to NEJM Knowledge+ Question of the Week
Managing Hereditary Hemochromatosis: An Expert Weighs In


One of the problems is the preconceived notion that only your answer is correct. There is often more than one way to treat a problem, and there is often controversy in the literature. Medicine is not like mathematics. There is not necessarily one correct answer. I have looked at a number of these questions (through NEJM Physician’s First Watch). The answers in many cases did not allow me to come away with a clearer understanding of disease processes or approaches to their diagnosis and management. In some cases, the reference were dated, ignoring more recent publications which did not share the same views.
Nonetheless, it is helpful to start somewhere.
However, at this point, the observation that the percentage of “correct” answers is low may be as much fault of Knowledge Plus as with the physicians answering the questions.
Thanks for your comments, Dr. Ball. We agree that there are controversies in medicine and that individual physicians might have reasons for straying from certain guidelines and recommendations, where the evidence is not particularly strong or there is a lot of ambiguity. However, it’s important that physicians understand what the current standards are in such cases, and we look to help ensure that knowledge.
Our questions are all designed to have multiple plausible answers but only one best answer for the scenario presented. This best answer is reviewed by several specialists before we approve it for inclusion in NEJM Knowledge+.
We recognize that a reader’s choice of an answer we deemed incorrect can sometimes indicate a problem with the question itself. We have a feature in NEJM Knowledge+ called “Challenge Us” that allows users to alert us whenever they think there’s a problem with a specific question. So far, we’ve heard from about 350 users, and we’ve evaluated each and every question they’ve challenged. In many instances, their comments have prompted minor edits that make the question or feedback clearer; very rarely have we needed to change the answer to a question. All of our edits are promptly incorporated into NEJM Knowledge+, so that users always have access to the most current version of our questions.
We strive to keep our reference lists up-to-date. In some instances, though, older references are still the best place to get a clear explanation of a given topic.
We hope you’ll continue participating in our Question of the Week, and if at any point, you find a problem with a question, by all means, let us know.
I have been certified in ABIM IM since 1973 (and 2 subspecialites) and have “re-upped” 3 times. All I want to know is if I do the NEJM MOCs (or whatever) can I then step up to the plate at 75 years? I no longer have a practice and live outside of the US 9 months of the year, while I spend the other 3 months at Vanderbilt University. I am interested in the contents (internal medicine) instead of the boilerplate you now insist upon.
I just want to take the test; I eschew all the other internet stuff, blogs, and whatever you now deem to be important for entertainment.
Yours,
Fred Luft
For the past six months I have been using Knowledge+ with UptoDate to prepare for my upcoming board examination. I, of course, won’t know if this strategy was effective until I take the boards. I have found some minor discrepancies between the 2 sources but not what I consider significant.
I have probably studied 15 hours per week and did not mind committing the time.
My problem is that overtime (I have < 3 years until retirement) my practice is very limited and I don't evaluate or treat many of the conditions I am being asked about, things like pulmonary alveolar proteinosis.
I wish there were a way to make it more relevant.
Also, I don't treat emergencies so if there is something I need to look up it is now at the push of a button so why all the memorization. Feels outdated.
I honestly dont care what is right or not because this is a test not real life. I would like to know how much will this prepare me for ABIM compare to the other competitions. I just want to know this…… Please just answer this, and I will buy your product
NEJM Knowledge+ delivers a personalized learning experience, powered by adaptive learning technology that continuously assesses your knowledge, confidence, and performance in real time. The product features thousands of case-based questions that have been vetted by both educators and clinicians. For an overview, see https://knowledgeplus.nejm.org/our-products/overview/
I used to be recommended this blog through my cousin. I’m now
not sure whether this submit is written by way of him as no one else know
such distinctive about my problem. You are incredible!
Thanks!